


Adaptation to Chronic Disease Risk

Millions of Americans have chronic health conditions and our health system spends billions on treating them. How can we configure incentives and markets to reduce the quality of life impact of these conditions on those afflicted and reduce the health cost burden on the greater economy?
I claim that the answer to this high stakes riddle is to empower individuals to invest in their own health. We need to lower the “Becker price” of health production and increase the skill of individuals in producing their own health.
Consider a slightly morbid thought experiment. The year is 1950 and a doctor tells you that you have Type 1 or Type 2 Diabetes. How much would you have been willing to pay at that point in time to not have these conditions? The year is 1960, same question. Repeat this thought experiment for each decade up until the present. I claim that a person’s willingness to pay (measured in $) to not have this condition is declining over time because we have an ever growing set of adaptation strategies including market products for nudging one to invest in self-protection of one’s health and other devices for monitoring the condition (blood sugar monitoring), drugs for treating the condition and medical procedures for dealing with the complications.
In a series of past papers, I have explored these ideas. In this Substack, I want to sketch out some Big Think related to the economics of adapting to chronic disease risk. Economists will see the links to the work of Gary Becker and James Heckman.
Matthew is born in 1966. When he is a teenager, he knows his grandparents and his parents and their coarse health history. He know what medical conditions are in the family genes. During the start of his life , he has built up skills (problem solving and grit) and he faces the usual temptations. He makes choices trading off current consumption and investment including investing in his health. Matthew’s maternal grandfather died from lung cancer and Matthew never smokes. This is an example of how our understanding of the family health history informs our choices today as we adapt to challenges we imagine we could face if we choose a given “fork in the road” such as starting to smoke. Rational addiction!
Matthew is 20 in 1986. There are no cell phones and no email. He goes to the library to learn things. If at age 27 in 1993, if Matthew is diagnosed with a chronic condition then he has fewer coping strategies than people have today to handle a similar diagnosis. Over time, we have an ever growing set of coping strategies to help us to adapt.
The interesting economics here pertains to whether we adapt to an anticipated risk (such as a pre-diabetes diagnosis) or ex-post —- once diagnosed.
With this preamble, I am now ready to discuss our new paper published in one of the JAMA journals.

Robert Kennedy Jr seeks to make Americans healthy again (MAHA). As an economist, I ask myself; why do we need his help? If we seek to be healthy, why can’t we achieve this goal on our own using market goods and our own time?
He would counter that the average American is aging and that the composition of our population is changing such that more of us have chronic conditions such as Type 2 diabetes, asthma, and high blood pressure and that more of us are obese.
Many health economists study how we spend as individuals and as a society in treating people who have these conditions. This doesn’t interest me that much.
What interests me is lifetime expectations and how our expectations shape our choices at different stages of life. If I know that 3 of my 4 grandparents have had type 2 diabetes, does this knowledge shape how I live my life? Do I exercise more and eat less to lower my risk? Or am I fatalistic and wait for my diagnosis under “business as usual”?
In our May 2025 paper, we focus on the following dynamics related to the U.S population.
Group #1 In the recent past, there were many undiagnosed diabetics (UDD) who did not know that they were (UDD). These individuals were not modifying their lifestyle because you are less likely to adapt to a condition you do not know about! The expansion of health care for the disadvantaged has offered the societal benefit of correctly informing people by giving them a diagnosis.
Notice a Jim Heckman selection point here, the “average diagnosed diabetic” changes over time as this group includes more poor people who in the past would not have been diagnosed.
Group #2 With the rising diagnosis of pre-diabetes, more and more highly educated people are being given an early “heads up” that they are at risk of being a Type 2 diabetic in the near future. Many in this group are responding to this information by adapting to chronic disease risk by losing weight, exercising more and changing their diet. This lowers their probability of becoming a diagnosed type 2 diabetic.
Do you see how these dynamics for group #1 and group #2 shift the composition of the “average diagnosed type 2 diabetic” over time. Researchers who study this group’s time trends over decades ignore this “apples and oranges” issue.

This New England Journal of Medicine paper is quite good but the authors ignore the microeconomic selectivity point. They implicitly assume that the probability of a person being a type 2 diagnosed diabetic is constant over time (controlling for one’s age, race and education).
We reject this implicit assumption.
Here is a write up of our recent paper . Here are some facts from our paper documenting health progress for diagnosed diabetics but little evidence of economic progress.
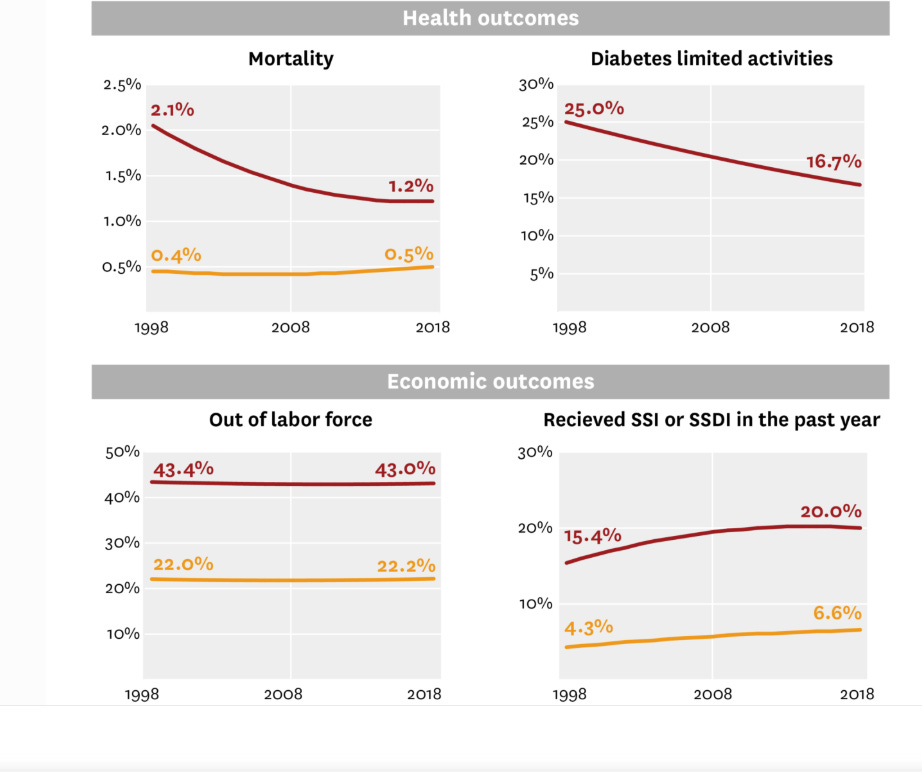

We are not passive victims in the face of new information regarding our health. The question arises of who has the self control and the resources to adapt to the challenge. These microeconomic factors determine what costs our health service system faces going forward.
I will expand on these points in future substacks.